 Motionnote
Motionnote
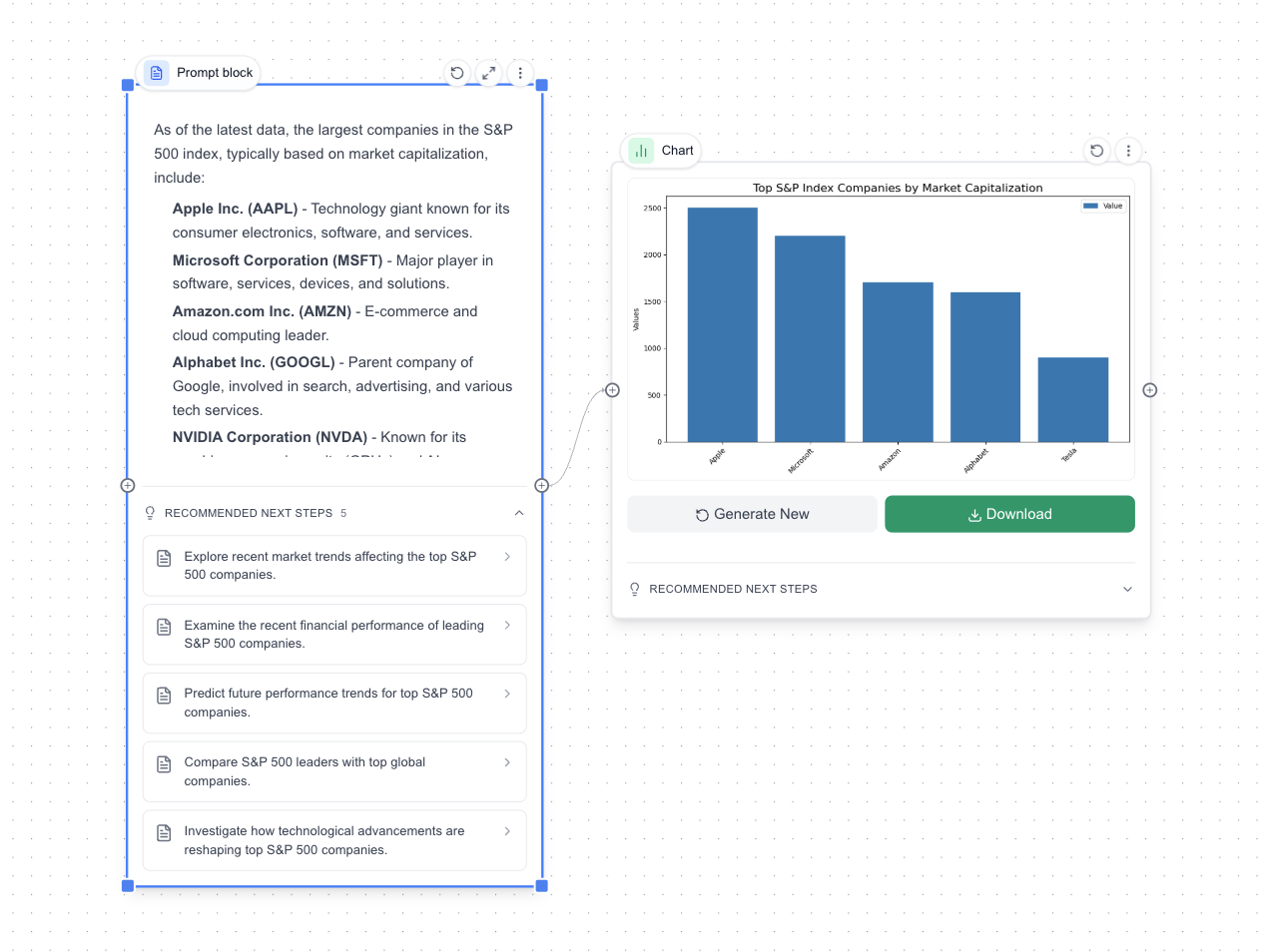
AI-powered word processor for creative minds — create images, video, and charts with AI inside your document.
Streamlining Team Documentation
I've been thinking about how our team can streamline the onboarding process for new‑hires. Right now, documentation is scattered across different tools, which makes it hard to find answers quickly. If we consolidate into a single hub and add more real‑world examples, I think it'll cut down on repetitive questions and help people ramp up faster.
I've been thinking about how our team can streamline the onboarding process for new‑hires. Right now, documentation is scattered across different tools, which makes it hard to find answers quickly. If we consolidate into a single hub and add more real‑world examples, I think it'll cut down on repetitive questions and help people ramp up faster.
 Awaken - AI Avatar
Awaken - AI Avatar Storyborrd
Storyborrd